Palliative T Spine 30Gy
IMRT SX1 A
 |
Rx: 30Gy/10fx
1:05 AP PA 2 field treatment delivery time
 |
 |
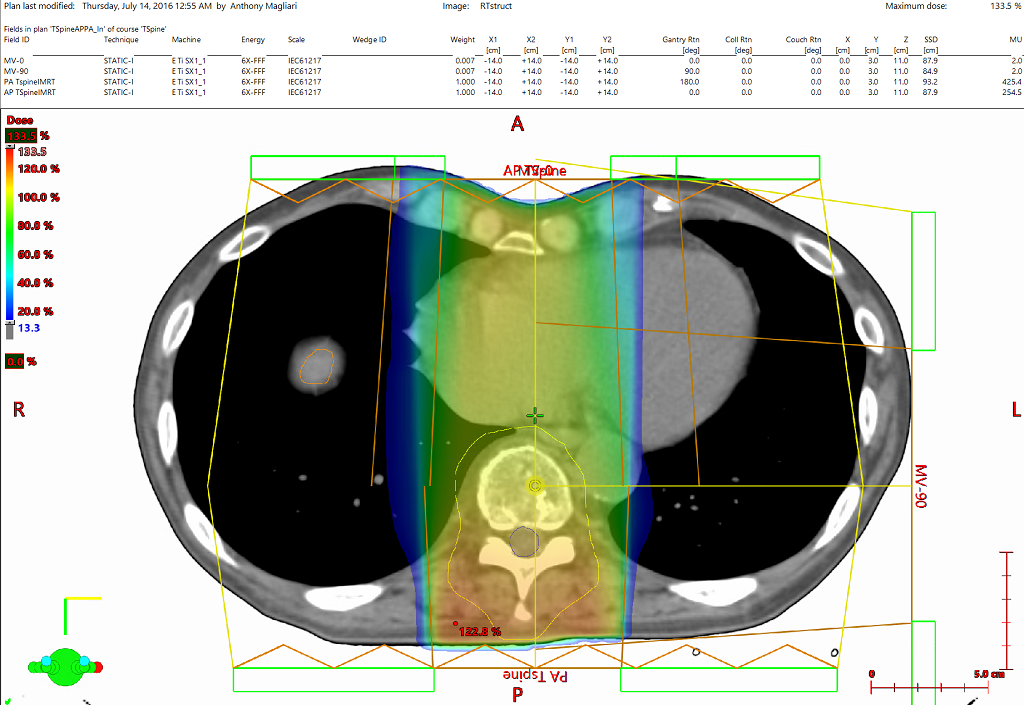
Due to the unflattened nature of the 6MV beam, traditional “2D” treatment techniques cannot be employed on most normal sized targets.
The inverse planning optimizer can be employed to deliver a homogenous dose distribution to the target, which requires a target volume. In this case the vertebra contours were drawn on just a few CT slices including the desired most superior and inferior slices and the rest of the CTV was created using interpolation. Then a small uniform expansion was created to make a PTV subtracting a (3mm) margin from the skin surface. Each plan was then optimized using only the PTV and Normal Tissue Objective (NTO). Optimization constraints used were as follows:
AP PA: PTV 100% 30.3Gy p140; PTV 0% 35Gy p110; NTO man p100 DTB1.0cm SD105% ED60% FO.05
Alternatively, the irregular surface compensator tool can be used to create a homogeneous dose at depth. This method would likely involve manual edits to the ideal fluence prior to plan approval thereby maintaining a completely forward planned workflow.
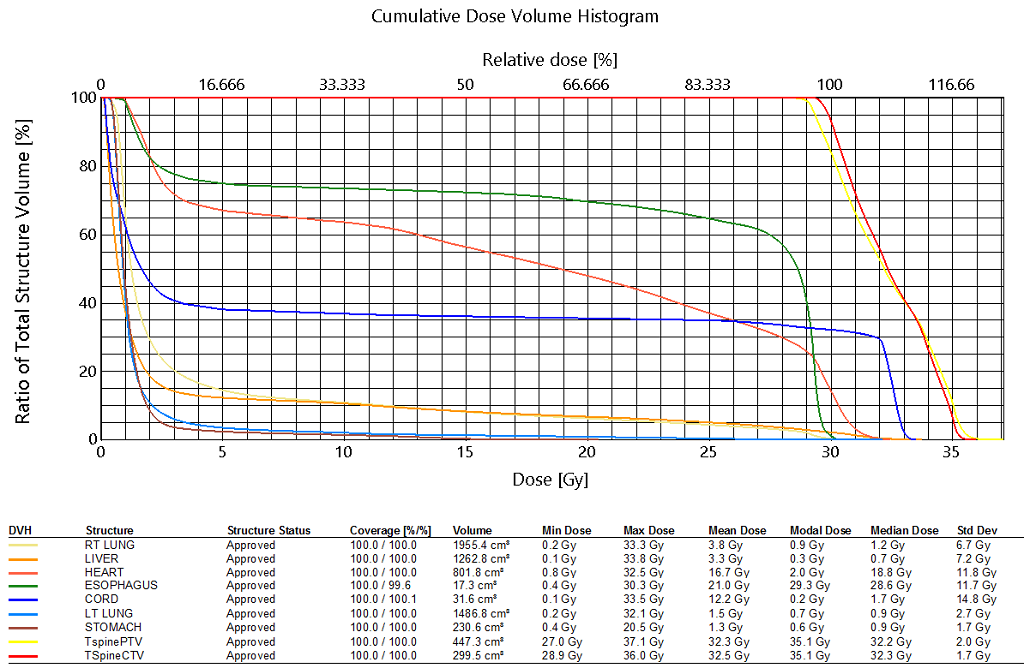
40Gy is too hot for the heterogeneity of this plan. I would favor more weighting on PA beam to decrease dose to the anterior structures which are not the target lesion. Coverage of the target lesion is good. I usually keep cord <35Gy and it appears that it may be >33Gy based on the isodose lines.
|
3rd party software plan report |
DICOM patient export |
Any reference to a "plan study" are simply what the organizers call each case and may not be a "study" in the FDA sense as they may not have been published in a peer reviewed journal.
Varian does not provide medical advice and these are illustrative examples only.
Leading plans by expert planner. Your results may vary.
FOR EDUCATIONAL AND SCIENTIFIC EXCHANGE ONLY – NOT FOR SALES OR PROMOTIONAL USE.