Lt Breast - Early Stage 50Gy (2014 AAMD / ROR Plan Challenge)
IMRT SX1
 |
 |
 |
Name (ID): ROQS-25, Breast-Simple (ROQS-25)
Plan or PlanSum ID: 3tang2SX1b
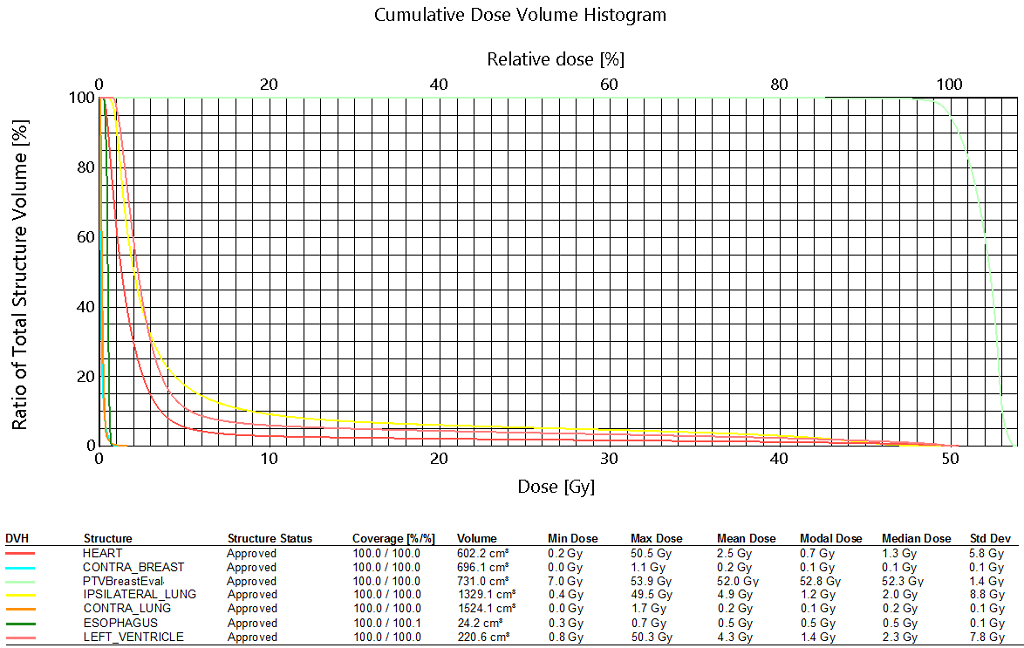
| Structure ID | Structure Code | Patient Structure | DVH Objective | Evaluator | Variation | Priority | Met | Achieved |
| BREAST_PTV_EVAL | PTVBreastEval40G | V50.0Gy[%] | >=95 | 90 | Variation | 94.49 % | ||
| LUMPECTOMY_PTV_EVAL | OrgLumpPTV | V50.0Gy[%] | >=99 | 95 | Goal | 100.00 % | ||
| BREAST_PTV_EVAL | PTVBreastEval40G | D50.0%[Gy] | <=52.5 | 56 | Goal | 52.324 Gy | ||
| BREAST_PTV_EVAL | PTVBreastEval40G | Max[Gy] | <=53.5 | 57.5 | Variation | 53.941 Gy | ||
| HEART | HEART | V10.0Gy[%] | <=3 | 10 | Goal | 2.83 % | ||
| HEART | HEART | Mean[Gy] | <=2 | 5 | Variation | 2.538 Gy | ||
| LEFT_VENTRICLE | LEFT_VENTRICLE | Mean[Gy] | <=4 | 10 | Variation | 4.276 Gy | ||
| IPSILATERAL_LUNG | IPSILATERAL_LUNG | V20.0Gy[%] | <=5 | 15 | Variation | 6.00 % | ||
| IPSILATERAL_LUNG | IPSILATERAL_LUNG | V10.0Gy[%] | <=7.5 | 20 | Variation | 9.10 % | ||
| IPSILATERAL_LUNG | IPSILATERAL_LUNG | V5.0Gy[%] | <=10 | 30 | Variation | 17.56 % | ||
| CONTRA_BREAST | CONTRA_BREAST | D0.03cc[Gy] | <=1 | 4.96 | Variation | 1.009 Gy | ||
| CONTRA_BREAST | CONTRA_BREAST | D5.0%[Gy] | <=0.25 | 1.86 | Variation | 0.412 Gy | ||
| CONTRA_LUNG | CONTRA_LUNG | V5.0Gy[%] | <=0 | 2 | Goal | 0.00 % |
 |
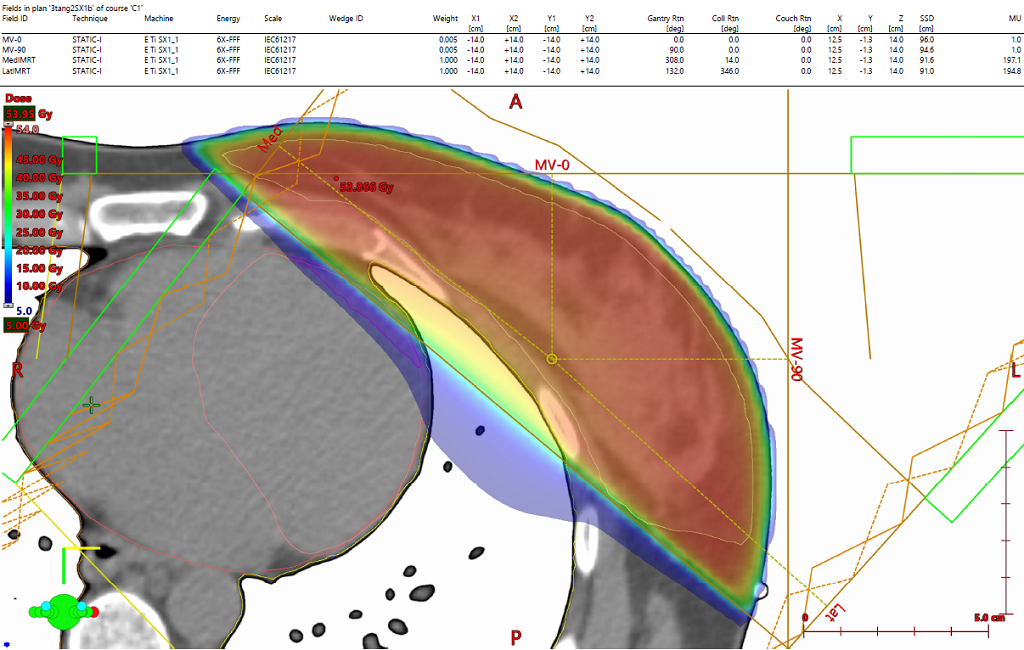
This plan consists of two slightly offset opposed fields (non-divergent to heart and lungs). First an initial fluence was created. This fluence can be created either using the inverse planning optimizer (with dose constraints entered for target and OARs) or by simply using the the irregular surface compensator tool (which maintains a forward planned workflow). The initial fluence was edited manually to: (1) create sharper dose gradients against the heart and lungs by deleting unnecessary fluence on the edges of the field and (2) decrease the max dose to the patient. The latter was accomplished by manually reducing fluence on each side of the target from its respective beam. Next, global plan normalization was adjusted to compensate for any target coverage lost due to the loss of fluence. This manual fluence editing process was repeated iteratively until the desired homogeneity was achieved.
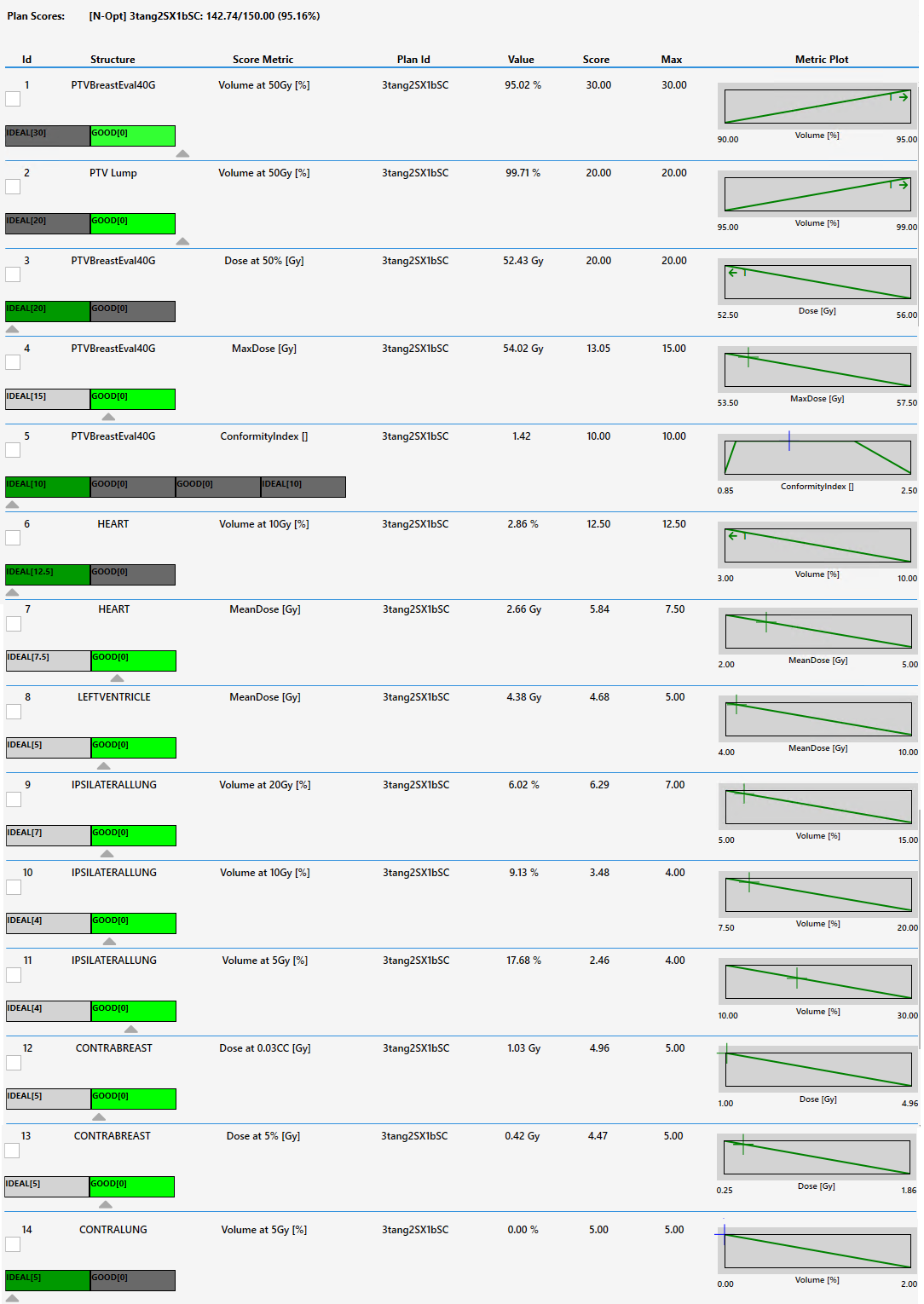
When manually editing the fluence edges of the field using the eraser tool in Eclipse, care must be taken because the eraser size is such that large sections of fluence may be deleted while using the tool. The precision offered by the eraser tool is not as fine as the setting of a fluence/field edge using a jaw or a max-leaf travel constraint that can be applied to other MLCs but is not available for the RDS system due to the design of the RDS MLC. In spite of the this limitation, this simple two field plan scored well relative to the plans submitted in the 2014 AAMD/ROR plan challenge where many of the highest scoring plans employed multi-field beam arrangements.
 |
|
3rd party software plan report |
Dosimetric ScoreCard |
Download patient export |
Any reference to a "plan study" are simply what the organizers call each case and may not be a "study" in the FDA sense as they may not have been published in a peer reviewed journal.
Varian does not provide medical advice and these are illustrative examples only.
Leading plans by expert planner. Your results may vary.
FOR EDUCATIONAL AND SCIENTIFIC EXCHANGE ONLY – NOT FOR SALES OR PROMOTIONAL USE.