Pancreas 52/46.8Gy (2012 AAMD / ROR Plan Challenge)
VMAT SX1
 |
Rx:52Gy/26fx to Pancreas and 46.8Gy to PTV
2012 AAMD / ROR Plan Challenge
![]()
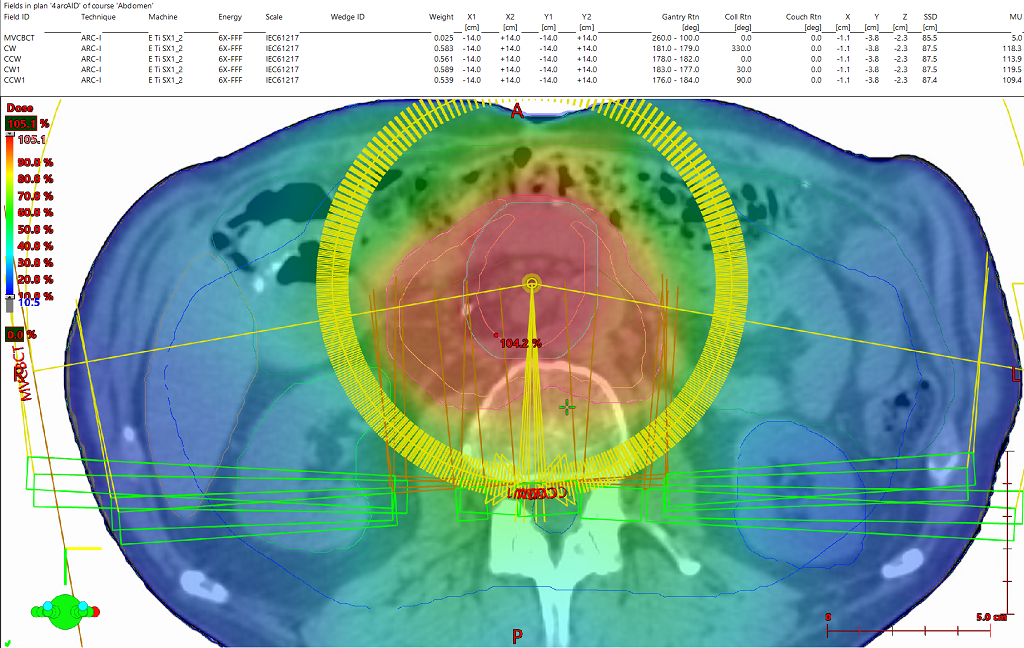
2:38 VMAT treatment arc delivery time
 |
 |
Name (ID): Z002442-ABD, AAPM (AAPM Z002442-ABD)
Plan or PlanSum ID: 4arcAID
| Structure ID | Structure Code | Patient Structure | DVH Objective | Evaluator | Variation | Priority | Met | Achieved |
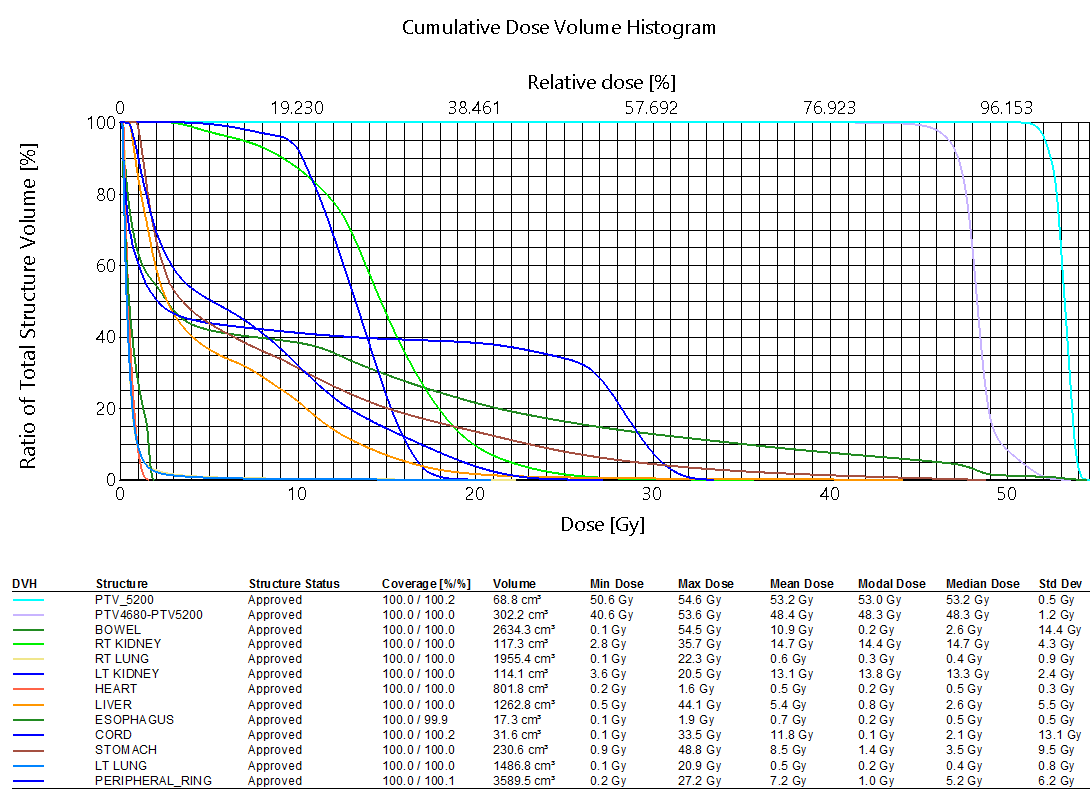
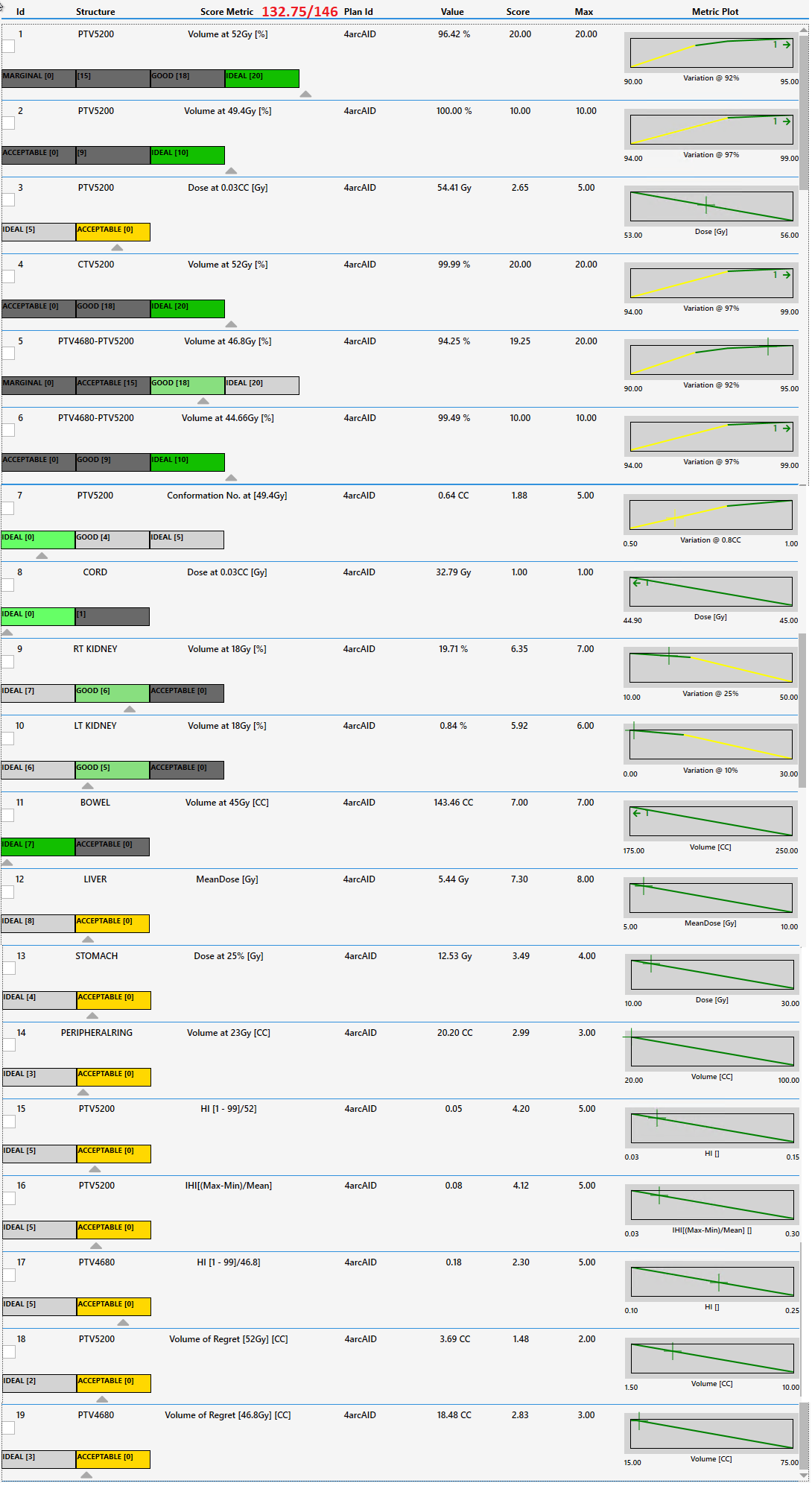
| PTV_5200 | PTV_5200 | V52.0Gy[%] | >=95 | 93 | Goal | 96.46 % | ||
| PTV_5200 | PTV_5200 | V49.4Gy[%] | >=99 | 97 | Goal | 100.00 % | ||
| PTV_5200 | PTV_5200 | D0.03cc[Gy] | <=53 | 56 | Variation | 54.409 Gy | ||
| CTV_5200 | CTV_5200 | V52.0Gy[%] | >=99 | 97 | Goal | 99.99 % | ||
| PTV4680-PTV5200 | PTV4680-PTV5200 | V46.8Gy[%] | >=95 | 93 | Variation | 94.37 % | ||
| PTV4680-PTV5200 | PTV4680-PTV5200 | V44.66Gy[%] | >=99 | 97 | Goal | 99.50 % | ||
| CORD | CORD | D0.03cc[Gy] | <45 | Goal | 32.780 Gy | |||
| RT KIDNEY | RT KIDNEY | V18.0Gy[%] | <=10 | 50 | Variation | 19.56 % | ||
| LT KIDNEY | LT KIDNEY | V18.0Gy[%] | <=0 | 30 | Variation | 0.81 % | ||
| BOWEL | BOWEL | V45.0Gy[cc] | <=175 | 250 | Goal | 142.95 cc | ||
| LIVER | LIVER | Mean[Gy] | <=5 | 10 | Variation | 5.437 Gy | ||
| STOMACH | STOMACH | D25%[Gy] | <=10 | 30 | Variation | 12.526 Gy | ||
| PERIPHERAL_RING | PERIPHERAL_RING | V23Gy[cc] | <=20 | 100 | Goal | 19.86 cc |
 |
The VMAT technique was chosen and 4 almost complete arcs were used. Each arc used a different start and stop angle (offset by 1 degree) to stagger the available control points throughout each arc rotation. Unique collimator rotations were selected per arc and ordered for fastest treatment delivery (330, 0, 30, 90). Zero degree collimator arc rotations make sense on this machine due to the reduced interleaf leakage of the two-stage, stacked and staggered MLC design. At first, VMAT would seem like the ideal technique to meet the challenging metric of no 50% of Rx dose (more than 3cm from the target anteriorly and 3cm from the skin surface elsewhere -- enforced by a “peripheral ring” metric in the scoring criteria). However, all efforts to improve upon the static field IMRT plan (utilizing VMAT technique) failed and this VMAT plan scored lower than the IMRT attempt, took slightly longer to deliver and took longer to optimize. From the CMD perspective the IMRT plan is the clear choice for this case.
Both pancreas RT plans were acceptable. The IMRT plan is slightly better. In both cases, the OARs, specifically the bowel. The homogeneity requirements are pretty tight and a priority in this case. These are achieved with good sparing of bowel and kidneys.
 |
|
3rd party software plan report |
Dosimetric Scorecard |
DICOM patient export |
Any reference to a "plan study" are simply what the organizers call each case and may not be a "study" in the FDA sense as they may not have been published in a peer reviewed journal.
Varian does not provide medical advice and these are illustrative examples only.
Leading plans by expert planner. Your results may vary.
FOR EDUCATIONAL AND SCIENTIFIC EXCHANGE ONLY – NOT FOR SALES OR PROMOTIONAL USE.